Degrees of Functional Abilities, Demystified
Learn the nuances that differentiate older adults based on functional ability so you can provide more targeted programming for individuals and groups.

If there is one word to describe the functional abilities of older adults, it’s “heterogenous.” Chronological age is only a rough guideline as to functional age (i.e., a person’s capabilities). Although functional capacity generally decreases with advancing age, the degree and rate of decline are highly variable, so individuals of the same age can exhibit highly variable levels of function. We probably all know 80-year-olds who can physically outperform many others 10 or 20 years their younger.
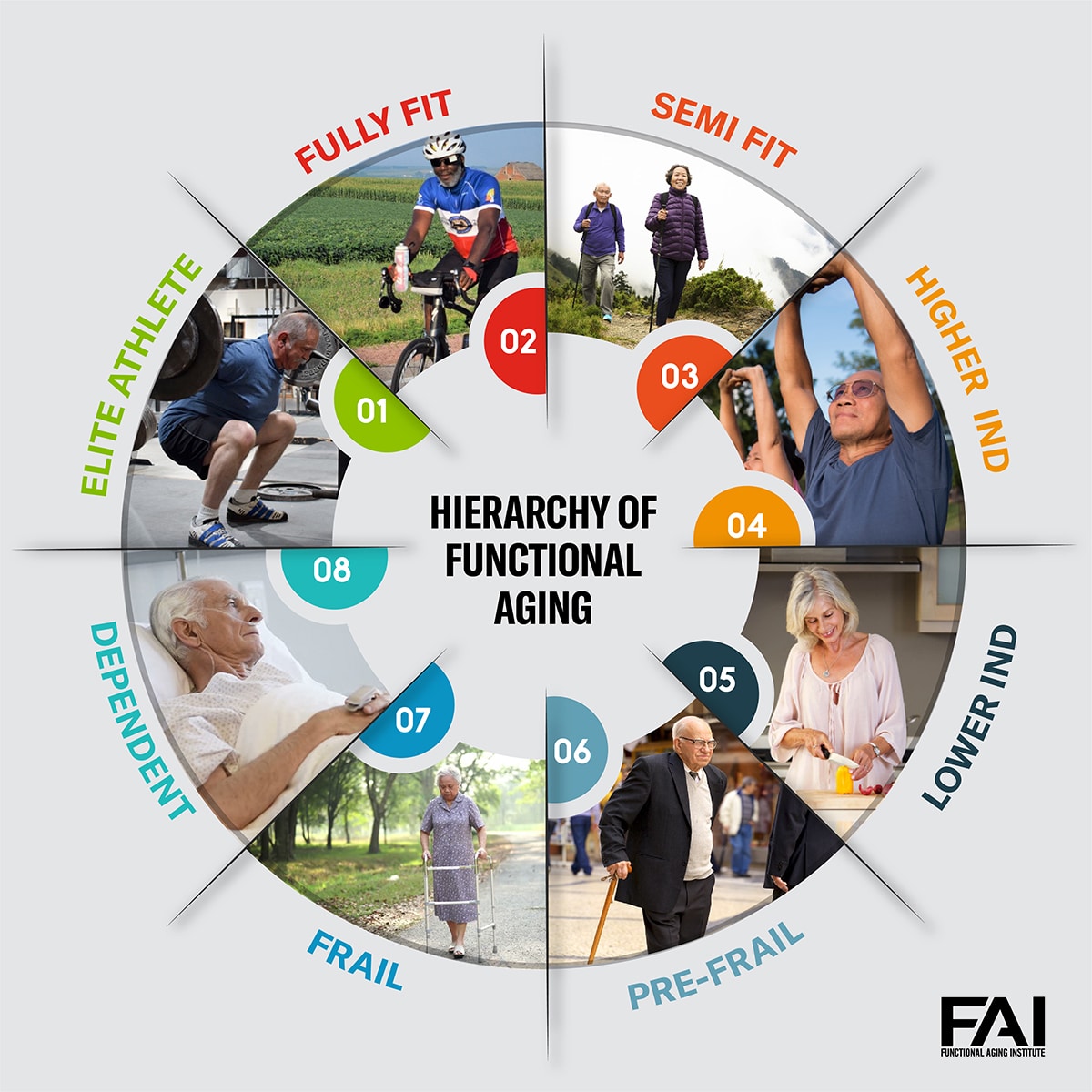
To help categorize the functional variability in the older adult population, the Functional Aging Institute (FAI) created the Hierarchy of Functional Aging model, right. The FAI model includes eight categories of functional abilities: dependent, frail, pre-frail, lower independent, higher independent, semi fit, fully fit and elite.
It’s important to note that this model represents a continuum of function, so even within each category there is variability. For example, two people categorized as higher independent may have very different scores within that category.
Additionally, individuals will vary considerably by functional abilities in where they excel or struggle in the Six Domains of Physical Function: balance, mobility, cognitive/emotional, neuromuscular, musculoskeletal and cardiorespiratory (right). A deficit in one or more domains can lead to struggles with performance of any type of activity at any level of fitness.
The Elite and Fully Fit Client
The physically elite older adult has achieved and maintained the highest levels of physical function, typically scoring in the top 1%–5% on functional and physical fitness tests for their age and gender. They are often more fit than many people who are decades younger.
They train rather intensely on a regular basis and often compete in tournaments, races and other events. This, along with typically excellent dietary habits, means they are typically in excellent health. However, this may depend on when they began exercising regularly. In the oldest age groups in competitive sports (85+ and 100+), there are many who did not start training until their 60s or 70s, while others began very young.
Fully fit older adults exercise primarily for health and well-being (not competition) and do so on a regular basis. Typically, their programs are less intense and time-consuming than those of elite athletes and, if they do sport-specific training, it is for enjoyment.
The fully fit also enjoy higher-than-average health and are seen as much younger than they are. They exceed others their age in almost every category of fitness, although not at the performance levels of the elite. They score in the top 5%–10% of performance for their age and gender.
Training
The focus for training elite and fully fit clients is on ensuring that they are training properly and safely for longevity. These groups can, and often do, engage in a wide variety of training modalities at a high level. It is important, therefore, that we ensure they are utilizing proper techniques and planning their training programs to avoid injury and overtraining. Factors such as nutrition, hydration, sleep and recovery should also be addressed, as they can impact performance.
See also: Training Techniques for High-Performance Masters Athletes
The Semi Fit Client
Unlike the fully fit, the semi fit excel in only one or two areas of fitness, usually because they exercise in only one modality. For example, swimmers or joggers may have high levels of cardiorespiratory fitness, but muscle strength and balance may be critically low.
Typically, the semi fit are also in good to excellent health, and they score in the top 5%–10% (for their age and gender) in one or two categories of fitness.
Training
Adding variety to your semi fit clients’ training programs is the priority, as they are already exercising consistently. Making time for other modes of training may necessitate cutting down on their preferred modality, which may be difficult for them. Use the Six Domains of Physical Function Model to expand their training.

The Independent Client
Higher independent individuals are physically active but may not exercise on a regular basis. If they do exercise, it is typically lower in duration, intensity and variability. Leisure-time activities may include walking, hiking, yardwork, gardening, tennis, golf and the like.
Their health may range from good to excellent, typically without serious debilitating disease, although they may be managing a chronic disease (which can cause a rapid physical decline if it progresses).
For the most part, they are fully functional, though their physiological and functional reserves are more limited than those in the categories above. Performance scores in this group are much more diverse than among fitter counterparts, ranging from average to somewhat above average. Their specific areas of need in the Six Domains of Physical Function also vary considerably.
Lower independent individuals are minimally active or sedentary. They typically choose hobbies and activities that require very little physical demand (such as reading). They score below average on most functional fitness assessments. They are at a higher risk of functional decline and are typically on a steeper downward functional trajectory than fitter individuals. The variability in impairments and chronic conditions is significant for this group.
Training
The strengths and deficits of higher and lower independent clients vary widely, even among those with similar functional abilities. One individual may have a deficit in strength and power, while another may be sufficient in these areas but low in balance and mobility.
It’s important to continually challenge these clients in new ways to help identify areas of struggle (the concept of “the exercise is the test”). For example, if you never have them perform a grapevine, then you may never discover that they struggle with this type of move.
From a musculoskeletal perspective, focus on the Seven Fundamental Movement Patterns: hinge, squat, lunge, gait/carry, anti-rotation, push and pull. Use isolated movements to address specific issues or goals, while encouraging them to become more active throughout the day.
See also: Functional Training for Active, Independent Living
The Pre-Frail and Frail Client
Pre-frail individuals are in a critical transitional stage between independence and frailty that’s characterized by meeting one or two of the five frailty criteria: unintended weight loss, muscle weakness, exhaustion or poor endurance, slow gait speed, and low levels of physical activity.
These individuals score lower than average on all functional fitness assessments and are on a steep downward functional trajectory toward frailty and dependence if the appropriate interventions are not made.
Due to their physical limits, it is difficult for them to engage in instrumental activities of daily living (IADLs), such as shopping, doing laundry and light housework, and preparing meals. Therefore, they continue to become less active and less engaged in all aspects of life. This can quickly become a downward spiral: Less activity leads to reduced physical abilities, which leads to less activity and so on.
Frail individuals meet three or more of the five frailty criteria mentioned on page 22. According to Campbell and Buchner (1997), frailty is a “condition or syndrome that results from a multi-system reduction in reserve capacity to the extent that a number of physiological systems are close to, or past, the threshold of symptomatic clinical failure. As a consequence, the frail person is at increased risk of disability and death from minor external stresses.”
Frail older adults can perform most or all basic activities of daily living (BADLs), such as bathing, dressing, transferring, toileting and feeding. However, they are typically unable to perform all the IADLs. Since many frail older adults have difficulty ambulating, the use of assistive devices (canes, walkers and rollers) is common.
These individuals are at high risk of an injurious fall and are more likely to have osteoporosis. They typically qualify for physical therapy due to their condition.
Training
Developing strength and power for frail and pre-frail clients is the priority, since sarcopenia (age-related loss of muscle mass and strength) is the central feature of frailty. While this group will have deficits in balance, mobility and gait, it is recommended to focus first on improving strength and power.
While it would be ideal to follow the Seven Fundamental Movement Patterns (hinge, squat, lunge, gait/carry, anti-rotation, push and pull), these individuals often lack the ability to perform them. Therefore, machine-based and isolated movements are recommended at first, followed by integrating whole-body functional moves.
For example, start with the leg press, leg curl and leg extension to facilitate a chair stand, which can then lead to a squat pattern. There will be a transitional time when you may be alternating between these movements from session to session. Shoot for a moderate- to high-intensity load for 8–12 repetitions. Also encourage regular physical activity outside of training, such as taking walks. They should build up to 30–60 minutes of moderate-intensity movement every day.
The Dependent Client
Dependent individuals are unable to perform all of the BADLs and are dependent on others and/or physical aids (e.g., canes, walkers, wheelchairs) to complete daily tasks. The extent of their physical disability is determined by the degree to which they cannot perform BADLs and IADLs. Disability rates increase with chronological age and are higher in females, African Americans and people living in poverty.
Keep in mind that individuals can move in and out of disablement, such as following a stroke (where function is lost) and during rehabilitation (where function is often regained). It is unlikely that a fitness professional will train dependent older adults unless they work in a nursing home or assisted-living facility.
See also: Pillars of Functional Training for Active Aging
How to Categorize Clients and Groups by Functional Abilities

You can typically determine an individual’s category quickly and rather accurately from asking questions and performing a few basic assessments, starting with a health history and the Physical Activity Readiness Questionnaire (PAR-Q).
This model can be extremely useful when creating small or large groups for training. Try to group individuals with similar levels of function but limit the span to one or two categories of function. For example, a group could include frail and pre-frail individuals (but not lower independent) or pre-frail and lower independent (but not frail).
Continuing to Explore the Continuum of Functional Abilities
While almost any kind of exercise is beneficial for older adults, taking the time to evaluate their functional abilities through their level on the Hierarchy of Functional Aging and address their deficiencies in the Six Domains of Physical Function will catalyze your effectiveness—and maximize their efforts.
Myths and Misconceptions
Sometimes preconceived notions allow individuals to become stuck at a level of functionality. Dispelling myths in clients and the fitness community can help prevent this.
Myths about the . . .
Elite and Fully Fit
- Their program is the best it can be.
- They are performing exercises properly.
- They are doing all the other things (nutrition, sleep, etc.).
Semi-Fit
- Because they are fit in one domain, they must be fit in all domains.
- What they are doing now is “good enough” since it is “better than nothing.”
- They don’t have major deficits that need to be addressed.
Higher and Lower Independent
- Their current activities are enough for functional longevity.
- They aren’t interested in exercising regularly.
- A generic program of cardio and strength training is all they need.
Frail and Pre-Frail
- It’s too late to make significant improvements.
- They are lazy and really don’t want to do more.
- They are far too unhealthy to work out, and it could be dangerous for them.
What About Chronic Conditions?
Addressing common chronic conditions and issues (such as osteoarthritis, osteoporosis, joint replacements and hypertension) is important but secondary to the individual’s functional status. Why?
Simply because all individuals need to be able to function well regardless of their chronic conditions.
Their specific conditions may require alterations to their movements and programming, for sure—but ultimately regular training is recommended for almost every type of condition, and for most there is little concern that training will be dangerous.
References
Campbell, A.J., & Buchner, D.M. 1997. For debate: Unstable disability and the fluctuations of frailty. Age and Ageing, 26, 315–18.
Spirduso, W.W. 1995. Physical Dimensions of Aging. Champaign, IL: Human Kinetics.
Cody Sipe, PhD
Cody Sipe is an associate professor and director of research at Harding University, co-founder of the Functional Aging Institute, and co-owner of Miracles Fitness. He has 20 years of industry experience as a trainer, manager, director, owner, teacher and researcher. As a recognized leader in functional fitness for older adults he has shared his expertise and cutting-edge approaches with thousands of fitness professionals around the world through numerous publications, international presentations and educational courses. His work has resulted in several awards including the 2005 IDEA Program Director of the Year.


