Addressing Exercise Barriers
A practical approach that will help trainers and clients alike.

Despite their best intentions, people struggle to be physically active due to exercise barriers. In fact, failing to translate good intentions into behavior is a lot more common than holding no intention of being active in the first place (Rhodes & de Bruijn 2013). Even those working with a personal trainer once or twice a week may avoid exercising outside of scheduled sessions, despite direction and encouragement from the trainer.
To assist clients in adhering to exercise routines, fitness pros need to understand the factors that influence behavior and have a system to help clients overcome exercise barriers. This article offers a practical approach.
What Determines Behavior and Exercise Barriers?
Motivation, opportunity and capability are the three determinants of behavior. If a client is motivated to do something, has the opportunity to do it and has the skill set it requires, the client will do the behavior (Michie, van Stralen & West 2011).
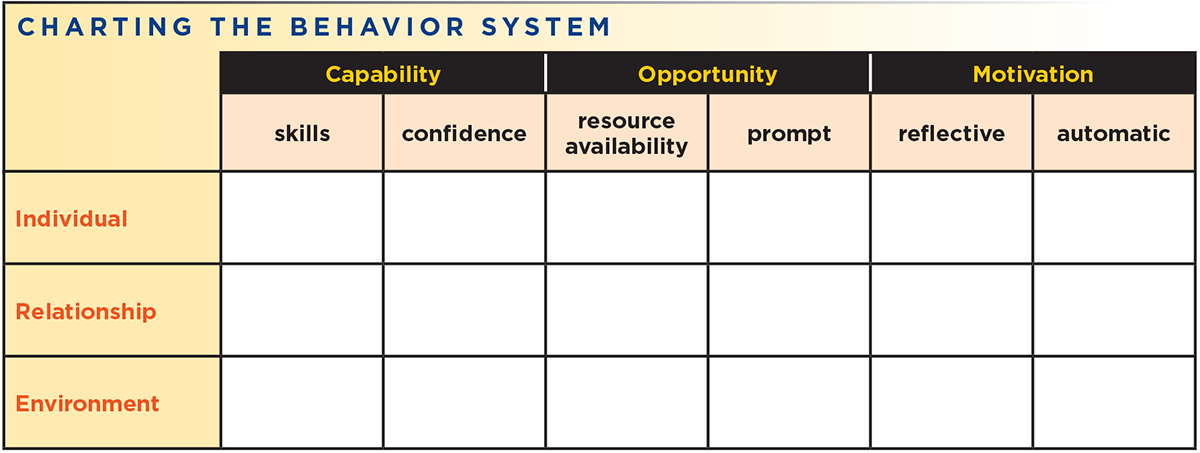
Susan Michie, FMedSci, FAcSS, professor of psychology at University College London, and colleagues refer to these determinants as the “Capability Opportunity Motivation” behavior system, or COM-B (Michie, van Stralen & West 2011). Capability refers to the physical and psychological capacity to do a behavior. Opportunity describes all the factors external to the individual that prompt a behavior or make it easier. Motivation comprises all the brain processes that influence behavior.
Capability has two subcomponents: physical (actual skills) and psychological (confidence to use those skills). Opportunity relates to availability and resources and also to prompts that can trigger the behavior. Motivation likewise has two subcomponents: reflective and automatic. The reflective part describes goal-setting, decision-making and planning, while the automatic part describes habit, identity, impulses and emotions (Michie, van Stralen & West 2011). These elements are shown in the chart below.

Using COM-B to Overcome Exercise Barriers
How do you apply the COM-B system with a client who is not adhering to exercise goals? To select the determinant that needs to be targeted, have the client examine the following six statements. Which statement(s) describe why the client struggled to act on good intentions?
- The task was too hard. (physical capability—skills)
- I lacked confidence that I could use the skills I have. (psychological capability—confidence)
- I did not have the resources to do the behavior. (opportunity)
- I did not remember to do the behavior. (prompt)
- I did not set a plan for when and where to do the behavior, or I did not have a plan to overcome barriers. (reflective motivation)
- I was more inclined to do something else. (automatic motivation)
Once exercise barriers are accurately identified, the next step is to understand what influenced each barrier.
See also: Motivational Interviewing: Talking Their Way to Health
Sources of Influence
From an ecological perspective, behavior is affected by multiple levels of influence. McLeroy and colleagues (1988) viewed behavior as being determined by intrapersonal factors (characteristics of the individual), interpersonal processes (social networks), institutional factors (social institutions), community factors (relationships among institutions within defined boundaries) and public policy.
For practical purposes, we’ll boil these down to three relevant areas of influence: the individual level, the relationship level and the environment. The individual level includes thoughts, beliefs and cognitions. The relationship level includes social networks. The environment includes home, work, school and neighborhood. Environment influences factors such as availability and accessibility.
Interventions should focus on all levels of influence. They must make an individual’s system work to get the results the person wants. When a well-intending client says he or she wants to do more physical activity but doesn’t follow through, an issue in the client’s system is causing the barrier.
The Behavior System
Integrating the social-ecological perspective with the COM-B framework completes the “behavior system.”
Cognitions, social networks and the structural environment all influence capability, opportunity and motivation, which in turn dictate behavior. The system is relevant for acting on good intentions and for continuing positive actions. With favorable system conditions, people are more likely to maintain a behavior change effort. If conditions are unfavorable at any point in the system, the weakness may thwart good intentions.
For example: If a client wants to run but has no friends who run, that person has a weak link at the reflective motivation–relationship level. Someone who wants to run but has no access to running trails has a weak link at the reflective motivation–environment level. And someone who wants to run but would rather watch television has a weak link at the automatic motivation–individual level.
If a client wants to change a behavior, ask which statements best describe their exercise barriers. Then ask what influenced each statement (cognitions, social networks or the environment). Where the issue lies reflects the weak point that needs to be addressed. Clients with a weak point in their systems will experience more barriers to physical activity, making them more likely to disengage from it.
See also: Group Fitness and the Stages of Behavior Change
Tailoring Behavior Change Techniques for Exercise Barriers

For a technique to be effective in overcoming exercise barriers, the source of influence needs to be addressed.
Behavior-change techniques (BCTs) are intervention components used to change the determinants of behavior. These techniques should either enhance motivation, opportunity or capability or reduce the need for what is lacking. BCTs are effective only if targeted to the relevant determinant. For instance, if confidence is the issue but motivation is targeted, the BCT will be inappropriately applied.
Kok et al. (2016) discuss parameters for effectiveness, the conditions that must be satisfied in practical application for the method to be effective (Kok et al. 2016). Through the COM-B series of questions, the client should be able to identify where the problem lies. For a technique to be effective, the source of influence then needs to be addressed.
Based on the behavior system proposed above (where the social-ecological perspective is integrated with the COM-B framework), BCTs can fit into any of 18 categories. Let’s take the example of someone who lacks the skill to do strength training and wants to harness a source of influence to make progress. The client might practice at home (individual level), hire a trainer (relationship level), or join a gym that promotes autonomy and relatedness (environment level).
If the client seeks out a personal trainer, the trainer will then tailor BCTs to the statement that best describes the client’s weak link. In these examples, each technique addresses the individual level of influence.
Statement #1: The task was too hard. (skills)
The capability determinant will cover true skill-related issues. For example, if a program called for running 13 miles or lifting 500 pounds, the client may have lacked the physical strength or stamina to complete the program. If the goal was to do vigorous exercise three times per week and strength training three times per week—and the client had not been exercising beforehand—the task demand was too high.
A solution is to reduce the task demand so the client feels confident about doing the behavior. Ask clients on a scale of 1–10 how confident they are that they can accomplish the exercise behavior they have selected. If the number is less than 8, reduce the difficulty of the task.
Statement #2: I lacked confidence that I could use the skills I have. (confidence)
With good programming, true capability barriers should not be an issue. Perceptions of inability to accomplish a task may be bigger problem.
A starter step is using a BCT that breaks down the sequence of events needed for a behavior to start. For example, a client may feel that doing an at-home training routine for 30 minutes is too much. The sequence of events that must happen for a client to do this may include putting on gym clothes, setting up weights and warming up.
A starter step reduces the friction of getting started by focusing on the first thing (or sequence of things) a client needs to do. If clients perceive capability as a barrier, ask them to identify their starter step and have them plan on doing just that. For example, instead of planning to work out, they just plan to put on gym clothes and get in the car. Or instead of planning to go for a 2-mile walk, they just plan to walk out the door. Once the starter step has been initiated, it should carry momentum toward the behavior.
Statement #3: I did not have the resources to do the behavior. (resource availability)
When people think of behavior in dichotomous terms, they fail to examine the multitude of choices they have. For example, they may think that if they do not have time to go to the gym, their opportunity to exercise is lost that day. They may also have an inaccurate perception of opportunity versus cost. Perhaps they think that if they exercise, they won’t have time to spend with their families or to watch a television show they like.
Encourage clients to stop thinking in limited terms and help them widen their options. Urge clients to examine all available exercise opportunities. If they do not have time to go to the gym, can they take a walk, do a body-weight circuit at home, follow a yoga video or go for a run?
Statement #4: I did not remember to do the behavior. (prompt)
Goals necessitate time management and specific plans to prompt the behavior. Consider two important forms of planning when implementing goals: action planning and habit stacking. Action planning describes when and where a behavior will happen. Habit stacking—an advanced form of action planning—involves pairing an existing habit with a behavior. This way, the old habit serves as the prompt for the new habit.
Statement #5: I did not set a plan for when and where to do the behavior, or I did not have a plan to overcome barriers. (reflective motivation)
It’s easy to act on good intentions when no problems get in the way. However, people run into barriers that can be demotivating. Coping planning is a self-regulation strategy that helps people act on their good intentions by identifying potential barriers and then making plans to work around those barriers. Barriers to exercise may include lack of physical energy, lack of mental energy or lack of time. Have clients identify what may get in the way, and then have them brainstorm possible solutions. Now ask them to select the solutions they believe will have the highest impact.
Statement #6: I was more inclined to do something else. (automatic motivation)
A frequent issue with health behavior is consistency. People may be forced to decide between doing what they want to do (relax on the couch) and doing what they should do (exercise). The conflict between immediate gratification and long-term results makes behavior change difficult (Milkman, Minson & Volpp 2014).
Temptation bundling involves pairing “want” activities (watching a television show, reading a book, having a delicious meal) with a behavior that provides benefits but requires self-regulation (exercising at the gym). To find the right pairing for exercise or physical activity, ask clients what they like. Maybe it is a podcast, audiobook or Netflix show. Have them pair the “want” with exercise.
Clearly, it is not advisable to watch a show during a resistance training session, so another option is to pair exercise with a contingent reward. For example, ask clients to agree that they can only watch their favorite show, get a pedicure or spend time with friends after they exercise.
See also: How to Create Outstanding Outcomes
References
Garon, J-D., Masse, A., & Michaude, P.C. 2014. Health club attendance, expectations, and self-control. Journal of Economic Behavior & Organization, 119, 364–74.
Kok, G., et al. 2016. A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychology Review, 10 (3), 297–312.
McLeroy, K.R., et al. 1988. An ecology perspective on health promotion programs. Health Education Quarterly, 15 (4), 351–77.
Michie, S., van Stralen, M.M., & West, R. 2011. The behaviour change wheel: A new method for characterizing and designing behavior change interventions. Implementation Science, 6, 42.
Milkman, K.L., Minson, J.A., & Volpp, K.G.M. 2014. Holding the Hunger Games hostage at the gym: An evaluation of temptation bundling. Management Science, 60 (2), 283–99.
Rhodes, R.E., & de Bruijn, G.J. 2013. How big is the physical activity intention-behaviour gap? A meta-analysis using the action control framework. British Journal of Health Psychology, 18 (2), 296–309.
Sallis, J.F., & Glanz, K. 2009. Physical activity and food environments: Solutions to the obesity epidemic. The Milbank Quarterly, 87 (1), 123–54.
Justin Kompf, MS, CSCS, CPT
Justin Kompf, MS, CSCS, CPT, is a PhD student at the University of Massachusetts at Boston, where he is studying exercise and health science with a focus on health behavior change. Find him at firstguessfitness.com.



