Do Ergogenic Aids Help or Hinder Athletic Performance?
Almost daily, people ask fitness professionals
about the latest and greatest dietary supplements
that claim to enhance physical performance.
Although it is outside the scope of practice of personal
trainers and fitness instructors ever to recommend
a particular ergogenic aid to anyone,
clients want to know if these products produce
the results promised in the ads. There is no denying
that dietary supplementation is widespread,
especially among professional and recreational
athletes. Frankly, it can be overwhelming even for
nutrition experts to keep up with all the news and
scientific research on every supplement that joins
the performance-enhancing arsenal.
In this article, we examine the current regulatory
state of the dietary supplement market and
define the different categories of these products.
We also take an in-depth look at four popular dietary
supplements in terms of their mechanisms
of action, side effects, safety and legality.
Our hope is that the information presented
here will give you more detailed knowledge of dietary
aids in general. While fitness professionals
are not permitted to prescribe dietary supplements
to clients, it is possible for you to be a
source of current and accurate knowledge about
such issues.
Concerns About Dietary Supplements
It is estimated that nearly 60% of all elite athletes use one or more
dietary supplements (Schroder et al. 2002). And people appear to
be using these supplements at an earlier age. Today, close to 45%
of collegiate athletes consume one or more dietary supplements,
most often multivitamin/mineral supplements and creatine (Beck
et al. 2006; Jonnalagadda,Rosenbloom & Skinner 2001). The two
critical questions most people ask about any dietary supplement
are always the same: Is the product safe? And is it effective?
So who is tasked with determining the safety and efficacy of dietary
supplements? In the past, the Food and Drug Administration
(FDA) regulated dietary supplements under the classification of
foods to ensure that these aids were safe for human consumption
and that package labeling was truthful and not misleading.
Unfortunately, that is no longer the case. In 1994, Congress enacted
the Dietary Supplement Health and Education Act
(DSHEA), which some experts say severely limits the FDA’s ability
to regulate these products (Barrett 2007).
By reclassifying dietary
supplements as a separate regulatory category from food
and drugs, the DSHEA essentially expanded the types of products
that could be marketed as supplements and allowed manufacturers
to propagate misleading information to consumers about
the effects of these aids (Barrett 2007).
As a result, many ingredients
used in dietary supplements are no longer subject to the
pre-market safety evaluations required of ingredients contained
in food or drugs. Many nutrition experts believe that the public
is now more vulnerable, because under the DSHEA there is no requirement
to prove claimed benefits of dietary supplements as
there is with drugs; no requirement to show safety with acute or
chronic administration; few provisions for quality assurance; and
liberal labeling requirements in relation to claims made.
Lack of Quality Controls
Quality control (which can be quite poor or even nonexistent
at many supplement companies) is a great concern for consumers,
who are at risk of ingesting a contaminated dietary supplement
or of not getting what they paid for in terms of product
quantity and potency. Evidence suggests that their concern is
well-founded. A few years ago, the International Olympic
Committee (IOC) laboratory in Cologne, Germany, raised concerns
when it reported the results of analyses carried out on several
legitimate dietary supplements (Maughan 2001).While none
of the tested supplements indicated on the product label that they
contained steroids and none cited any safety warnings, the lab
identified the presence of nandrolone, testosterone and other
steroids (Maughan 2001).
When the same lab followed up this study with a larger survey
involving 634 different product samples purchased from 13
countries around the world, the results were equally dire
(Maughan 2001). They showed that 94 of the supplements
(14.8% of the products analyzed) contained substances prohibited
by the IOC.While the brand names of the tainted supplements
were not published, the sampling included vitamins and
minerals, protein supplements, creatine and other popular products
(Maughan 2001).
To address this concern, the FDA has issued a new rule requiring
manufacturers of dietary supplements to follow “current
good manufacturing practices”(FDA 2007). The rule is designed
to ensure that dietary supplements are produced in a “quality
manner, do not contain contaminants or impurities, and are adequately
labeled” (FDA 2007).While this is a positive development
for consumers, the new requirement has a 3-year phase-in,
which won’t be complete until June 2010, according to the FDA.
What’s more, the new rule does not require manufacturers to
prove the efficacy and safety of any dietary supplement. That’s
why consumers still need to remain vigilant about any supplements
they use. Athletes, coaches, personal fitness trainers and
other health providers must know of the inherent risks associated
with taking any supplement, from a simple multivitamin to
a purported performance-enhancing product.
Defining Terms
The FDA legally defines a dietary supplement as follows: “a product
that is intended to supplement the diet that bears or contains
one or more of the following ingredients: a vitamin, a mineral,
an herb or other botanical, an amino acid, a dietary substance for
use by man to supplement the diet by increasing the total daily
intake, or a concentrate,metabolite, constituent, extract or combination
of these ingredients” (FDA 1995).Under the DSHEA, a
dietary supplement is adulterated if it or one of its ingredients
presents “a significant or unreasonable risk of illness or injury”
when used as directed on the label, or under normal conditions
of use (if there are no directions) (FDA 1995).
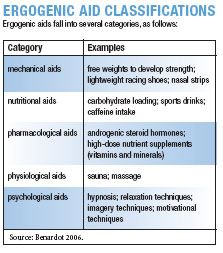
Dietary supplements are an umbrella for a wide range of
products, including weight loss pills and substances that promise
to increase physical performance. Ergogenic aids are a type of
dietary supplements that can increase the capacity for bodily or
mental labor, especially by eliminating fatigue symptoms. These
aids fall into different categories: mechanical aids, nutritional
aids, pharmacological aids, physiological aids and psychological
aids (see “Ergogenic Aid Classifications” chart).
Nutritional ergogenic aids refer to substances that enhance
performance and are either nutrients, metabolic byproducts of
nutrients, food (plant extracts) or substances commonly found
in foods (caffeine and creatine) that are provided in amounts
more concentrated than normally occur in the natural food supply
(Benardot 2006).
The following sections discuss some of the four most popular
types of supplements used to enhance physical performance:
caffeine, creatine, carnitine and amino acids.
Caffeine
Caffeine is one of the most widely consumed drugs in the world.
Because it is cheap, medically safe and socially acceptable, it has
become a popular ergogenic aid for athletes (Antonio 2004).
What’s more, it has recently been removed from the IOC’s
banned-substance list, which will likely make it even more widely
used and available to athletes (Beck et al. 2006).
Caffeine works as a central-nervous-system stimulant and a
muscle relaxant. There is much scientific research to suggest that
caffeine is an effective ergogenic aid for increasing endurance exercise
performance, anaerobic performance and muscle strength
(Beck et al. 2006). The possible mechanism of action for the increase
in endurance performance may lie in the fact that caffeine
increases the concentration of free fatty acids (FFAs) in plasma;
it is thought that this increased availability of FFAs may enhance
the ability of the cell to use these fats as fuels in endurance-type
low-intensity exercises (Spriet 1995).
There is also widespread research to prove the positive ergogenic
effects of caffeine on endurance performance, either by
increasing oxygen consumption or by improving performance
times (Bell & McClellan 2003). One study found that caffeine had
a positive impact on the performance of male distance runners:
the group of caffeine drinkers who consumed 1.4 milligrams
(mg) of caffeine per pound of body weight showed a 1.2% improvement
in an 8K race (Birnbaum & Herbst 2004). Another
study found that caffeine was equally effective during cycling
bouts. In this case, caffeine ingestion significantly increased the
riders’ exercise time to exhaustion, and repeating the dose after
exhaustive exercise was not necessary to maintain the ergogenic
effect 5 hours later (Engels et al. 1999).
While studies on caffeine have previously shown its benefit
for increasing endurance-exercise performance, new research
is proving the aid’s positive effects on anaerobic
performance and muscle strength. For example, a recent study
that examined whether caffeine could improve cyclists’ times
during a 1-kilometer sprint reported a 3.1% improvement
with the caffeine group (Wiles et al. 2006). Another study reported
a significant increase in 1-repetition maximum bench
press for participants who took a caffeine supplement prior
to exercise (Beck et al. 2006). Caffeine may be an effective supplement
for increasing upper-body strength and could be used
by elite athletes for competition or by recreational athletes for
resistance training.
Before you reach for that cup of java, keep in mind that caffeine
is not the answer to everyone’s need for power or speed.
It is unsuitable for growing children or adolescents, especially.
There is also a body of research that has failed to show any positive
effect, either aerobic or anaerobic, from consumption of
caffeine (Ahrens et al. 2007; Crowe, Leicht & Spinks 2006;
Lorino et al. 2006).
Safety/Side Effects of Caffeine
While caffeine is generally considered safe, it is important to note
that there have been reports on caffeine toxicity. In one case, a
16-year-old male who ingested an estimated 6–8 grams (g) of caffeine
manifested many of the adverse effects seen with acute caffeine
ingestion, such as elevated blood glucose, tachycardia and
agitation (Leson,McGuigan & Bryson 1988).
With caffeine, as with any drug or supplement, there is the potential
for abuse and misuse. A recent cover story in U.S. News
& World Report cited the increased use and abuse of caffeinated
drinks such as Red Bull, especially among adolescents (Shute
2007). The growing appeal of high-octane energy drinks has had
some officials concerned enough to act. The FDA recently sent a
warning letter to Redux Beverages LLC of Las Vegas—the manufacturer
of Cocaine Energy Drink—for marketing the beverage
“as an alternative to an illicit street drug.” The company’s own
website used the terms “cocaine—instant rush.” [Editor’s note: In early May, the product was pulled from shelves nationwide; the
company reintroduced the drink under a new name in mid-June.]
Elsewhere, a high school in Colorado Springs, Colorado, recently
banned a drink called Spike Shooter after two students
were taken to the hospital complaining of nausea, vomiting and
heart palpitations after drinking an 8-ounce can, which contains
300 mg of caffeine (Shute 2007).
With plenty of data now available about the ergogenic benefits
of caffeine, it is highly likely that we will see more of these
products flooding the market. Expect increased consumption of
such drinks in the future.
Creatine
Creatine is one of the most popular dietary supplements used to
enhance athletic performance (Bemben & Lamont 2005).
Creatine is synthesized from amino acids in the liver, pancreas
and kidneys at a rate of 1g per day (g/dy). Creatine is also consumed
in sources such as meat and fish. Skeletal muscle holds
95% of the 120–140 g creatine found in the body. In the muscle,
creatine is converted into phosphocreatine, necessary for production
of adenosine triphosphate (ATP), which provides an
anaerobic source of energy (McArdle, Katch & Katch 1999).
Creatine ingested through supplementation is reportedly absorbed
into the muscle exclusively by means of a creatine transporter,
called CreaT1 (Schoch,Willoughby & Greenwood 2006).
Phosphocreatine is the major source of muscle energy during any
exercise bout lasting 2–30 seconds. The availability of phosphocreatine
is believed to become a limiting factor during short bouts
of high-intensity exercise. Therefore, it is thought that if more
phosphocreatine is available via creatine supplementation, there
will be a faster recovery of ATP, thus improving high-power activity.
The ergogenic claims of creatine supplementation include
increased strength, power output and changes in fat-free mass.
The most common loading program cited in the research is an
initial loading phase of 20 g/dy for 5–7 days, followed by a maintenance
phase of 3–5 g/dy for differing periods of time (1 week to
6 months) (Bemben & Lamont 2005). More recently, a new dosing
strategy has been introduced, which is based on either total
body mass or fat-free mass and which yields approximately 20
g/dy (Schoch,Willoughby & Greenwood 2006).This strategy suggests
that creatine uptake will differ in regard to differences in
muscle mass, perhaps owing to the CreaT1 uptake mechanism.
It is thought that CreaT1 activity is lower in certain people
known as “nonresponders.” A study that compared the traits of
creatine supplement responders and nonresponders found that
responders generally
• had lower initial quantities of intramuscular creatine and were
able to absorb and take up greater amounts via supplementation;
• had a greater percentage of type II muscle fibers;
• had larger muscle fiber cross-sectional areas; and
• had more fat-free mass than the nonresponders (Syrotuik &
Bell 2004).
These findings suggest that the efficacy of creatine supplementation
may lie in one’s biological profile.
Scientific studies have consistently demonstrated the efficacy
of creatine supplementation for increasing muscular strength,
power output and body mass during short, repeated bouts of
maximal exercise in healthy, untrained young adults (Bemben &
Lamont 2005; Greenwood et al. 2000; Schoch,Willoughby &
Greenwood 2002). However, about half of all the published research
on creatine has failed to show any ergogenic effect in this
population. Specifically, creatine supplementation does not appear
to enhance endurance activities.
Since it has been fairly well established that creatine does increase
muscular strength and power in healthy young males,
researchers are now turning to other populations to determine
whether creatine improves their physical performance as well.
One study tested the effect of 2 and 5 days of creatine loading on
anaerobic working capacity in women athletes vs. a placebo
group; results showed an increase in anaerobic work capacity
of 22% after the 5-day loading phase (Eckerson et al. 2004).
So what are the practical ramifications of taking creatine
to improve physical performance? According to Jay Hoffman,
PhD, a professor at The College of New Jersey, “The efficacy
of creatine supplementation has been well established in an
athletic population. However, there need to be some additional
studies examining various loading schemes and appropriate
intake amounts for individuals of varying body masses
and age ranges.”
Safety/Side Effects of Creatine
The safety of creatine has been hotly debated. Although the general
consensus is that creatine is safe, there is scant evidence on
its effect in adolescents or the ramifications of its long-term use.
Anecdotal reports of the side effects of creatine supplementation
include gastrointestinal disturbances, muscle cramps, weight gain
and nausea (Leson,McGuigan & Bryson 1988).
Research continues to support the use of creatine for improved
performance, but results may vary depending on the individual’s
biological profile.Appropriate dosing strategies should
be implemented to increase the potential benefits and reduce any
possible side effects. Adding creatine to a carbohydrate source
has been observed to enhance uptake via an insulin response
(Green et al. 1996).
Carnitine
Carnitine is another popular ergogenic aid used by consumers.
Manufacturers claim that carnitine supplements can decrease
muscle pain and increase weight loss, endurance, cardiovascular
function and strength.
L-carnitine was first discovered in muscles in the early 1900s.
Carnitine plays a critical role in energy production; it transports
long-chain fatty acids into the mitochondria cells so they can be
burned to produce energy.Approximately 95% of the body’s carnitine
stores are in the skeletal and cardiac muscle (Fragakis
2003). Carnitine occurs in two forms, known as D and L, which
are mirror images of each other. Only L-carnitine is active in the
body and is the form found in food.
Healthy adults and children do not need to consume carnitine
from food or supplements, because the liver and kidneys
produce sufficient amounts from the amino acids lysine and methionine
to meet their daily needs.
While more and more athletes are turning to carnitine to improve
performance, there is no consistent evidence that carnitine
supplements can enhance exercise or physical performance in
healthy subjects. However, recent studies have found some improvements
in recovery from resistance exercise when carnitine
is taken at a dose of 1–2 g/dy (Spiering et al. 2007).
Safety/Side Effects of Carnitine
No serious adverse effects have been reported with carnitine
doses ranging from 0.5–0.6 g/dy (Fragakis 2003). Most study
protocols have used an oral dose of 2–4 g/dy, which is the typical
recommendation from manufacturers. Higher doses (i.e.,
more than 6 g/dy) have been associated with nausea and diarrhea
(Fragakis 2003).
Amino Acids
It has been well documented that endurance-and strength-trained
athletes need more protein than their more sedentary
counterparts. However, it has been equally well documented that
this increased protein intake can be achieved through diet alone.
To clarify these needs, the American Dietetic Association
(ADA), the Dietitians of Canada (DC) and the American College
of Sports Medicine (ACSM) co-wrote and released a joint
Position Paper on nutrition and athletic performance in which
they recommended that strength athletes consume 1.6–1.7 g protein
per kilogram of body weight (kg/bw) and that endurance
athletes need 1.2–1.4 g protein/kg/bw (ADA, DC & ACSM 2000).
But since amino acids (AAs) are the building blocks of protein,
can taking an AA supplement help with muscle building?
With 20 different amino acids in dietary protein, researchers have
been working overtime to determine whether specific amino
acids can help prevent fatigue, act as an ATP-sparing mechanism
during exercise, increase the secretion of anabolic hormones or
reverse/prevent the effects of overtraining.
One study did find a net positive increase in muscle protein
balance in subjects who consumed about 0.1 g of essential amino
acids per kg/bw during the first few hours of recovery from heavy
resistance exercise (Gibala 2002). According to one researcher,
providing an ample supply of essential amino acids to the muscle
1–3 hours before or after exercise may help to further muscle
protein synthesis (Williams 2005).
Amino acid cocktails seem to be a topic of current research;
scientists are mixing AAs with protein, carbohydrate and other ergogenic
aids, such as creatine, to see if there is enhanced benefit.
Due to space constraints, we cannot address all AAs. Instead,
we’ll focus on a few of the most popular: branched-chain amino
acids, glutamine and arginine.
Branched-Chain Amino Acids
Isoleucine, leucine and valine make up what are known as the
branched-chain amino acids (BCAAs), a group of essential
amino acids that have been studied for their potential role in delaying
central-nervous-system fatigue in athletes. However, much
of the existing research on BCAAs is inconclusive, and more studies
are needed to determine the mechanism of action, efficacy
and safety of these AAs.
Glutamine
Glutamine is a nonessential amino acid, meaning that it can be
produced in the body; it is also the most abundant free amino
acid in skeletal muscle and plasma. The rationale for glutamine’s
use as an ergogenic aid comes from a study that found that this
AA effectively counteracted protein synthesis decline and muscle
wasting from repeated use of glucocorticoids (McArdle,Katch
& Katch 1999).
During times of stress, the body’s need for glutamine can exceed
its supply. This has led scientists to theorize that supplemental
glutamine may help with recovery from the stress of
exercise. However, research on glutamine supplementation has
not yielded convincing evidence that this product provides any
ergogenic effect.
Arginine
Arginine is a nonessential amino acid involved in the synthesis
of urea in the liver.However, during periods of growth the body
may need more arginine than is available because arginine is
thought to stimulate the secretion of anabolic hormones, such
as human growth hormone (HGH) and insulin (Fragakis 2003).
Given its apparent role in increasing HGH levels, arginine may
possibly enhance muscle building. At this time, it remains unclear
whether arginine supplementation has any true ergogenic
benefit. However, some studies have shown that arginine may
hold promise for wound healing and for improving cardiovascular
health in patients with heart disease.
Safety/Side Effects of Amino Acids
Individuals who are prone to kidney stones or at risk for kidney
disease should consult their physician prior to increasing the
amount of protein in their diet.While most AA supplements are
considered safe, any supplement is subject to impurities or to the
lack of quality assurance mentioned earlier.
Supplement Summary
This article did not set out to cover the full breadth of research
available on each supplement highlighted. Rather, the purpose
was simply to provide a general understanding of the current
research on different dietary supplements; to explain the lack
of government regulation; and to issue the reminder that fitness
professionals need to stay within their scope of practice when it
comes to discussing ergogenic aids with clients.
That said, it is important for fitness professionals to be able
to discuss these aids in an educated and impartial manner, if only
to remind clients of the potential dangers and ramifications of
supplement use.
Supplements at a Glance
Need a pocket-sized guide to remember some of the supplements covered in this article?
| Supplements | Potential Action | Research Findings | Side Effects | Legal Status | ||||
|---|---|---|---|---|---|---|---|---|
| caffeine | increases muscles contractility; improves aerobic endurance; improves fat metabolism |
consistent benefits shown | mild | legal | ||||
| creatine | improves repeated high-intensity activity endurance |
benefits shown, but no safety data available for teens | none in short term; unknown in long term | legal | ||||
| carnitine | increases fat metabolism | research still inconclusive, but recent findings consistent in showing improved recovery from resistance training | none | legal | ||||
| amino acids | delay fatigue; increase secretion of anabolic hormones | research inconclusive, but athletes do benefit from proper protein intake and timing | none | legal |

Ellie Huff, RD, CSCS, and Dale Huff, CSCS, are co-owners of
NutriFormance LLC and NutriFormance Acceleration LLC, based in
St. Louis, Missouri. They can be reached at www.nutriformance.com
for questions.
Resources
Here are some of the most reliable sources for credible and
current information on dietary supplements:
ConsumerLab.com LLC, www.consumerlab.com
MedlinePlus (information on drugs, supplements herbs),
www.nlm.nih.gov/medlineplus/druginformation.html
Office of Dietary Supplements, National Institutes of Health,
http://ods.od.nih.gov
Supplement Watch, www.supplementwatch.com
USDA Center for Food and Applied Nutrition, Center for Food and
Applied Nutrition, www.cfsan.fda.gov/~dms/ds-savvy.html
Birnbaum, L.J., & Herbst, J.D. 2004. Physiological effects of caffeine on cross-country
runners. The Journal of Strength and Conditioning Research, 18 (3), 463–65.
Crowe,M.J., Leicht, A.S., & Spinks,W.L. 2006. Physiological and cognitive responses
to caffeine during repeated, high-intensity exercise. International Journal of Sport
Nutrition and Exercise Metabolism, 16 (5), 528–44.
Eckerson, J., et al. 2004. Effect of two and five days of creatine loading on anaerobic working
capacity in women.The Journal of Strength and Conditioning Research, 18(1), 168–73.
Engels, H.J., et al. 1999. Influence of caffeine on metabolic and cardiovascular functions
during sustained light intensity cycling and at rest. International Journal of Sport
Nutrition, 9 (4), 361–70.
Food and Drug Administration (FDA). 1995.Dietary supplement health and education
act of 1994. Center for Food Safety and Applied Nutrition. www.cfsan.fda.gov.
Food and Drug Administration (FDA). 2007. FDA issues dietary supplements final rule.
Center for Food Safety and Applied Nutrition. www.fda.gov/bbs/topics/NEWS/
2007/NEW01657.html.
Fragakis, A.S. 2003. The Health Professional’s Guide to Popular Dietary Supplements.
American Dietetic Association.
Gibala, M. 2002. Dietary protein, amino acid supplements, and recovery from exercise.
Sports Science Exchange, 15 (4), 1–4.
Green, A.L., et al. 1996. Carbohydrate ingestion augments skeletal muscle creatine accumulation
during creatine supplementation in humans. American Journal of
Physiology, Endocrinology and Metabolism, 271, E821–26.
Greenwood, M., et al. 2000. Creatine supplementation patterns and perceived effects in
select Division I collegiate athletes. Clinical Journal of Sport Medicine, 10 (3), 191–94.
Jonnalagadda, S.S., Rosenbloom, C.A., & Skinner, R. 2001. Dietary practices, attitudes,
and physiological status of collegiate freshman football players. The Journal of Strength
and Conditioning Research, 15 (4), 507–13.
Leson, C.L.,McGuigan, M.A., & Bryson, S.M. 1988. Caffeine overdose in an adolescent
male. Journal of Toxicology—Clinical Toxicology, 26 (5–6), 407–15.
Lorino, A.J., et al. 2006. The effects of caffeine on athletic agility. The Journal of Strength
and Conditioning Research, 20 (4), 851–54.
Maughan, R. 2001.Dietary supplements:Contamination may cause failed drug tests.Gatorade
Sports Science Institute Hot Topic Article.www.gssiwebde.com/reflib/refs/32/may2001.
McArdle,W., Katch, F., & Katch, V. 1999. Sports & Exercise Nutrition. Philadelphia:
Lippincott,Williams & Wilkins.
Poortmans, J.R., & Francaux, M. 2000.Adverse effects of creatine supplementation: Fact
or fiction? Sports Medicine, 30 (3), 155–70.
Rebouche, C.J. 1999. Carnitine. In M.E. Shils, J.A. Olson, M. Shike, & A.C. Ross (Eds.),
Modern Nutrition in Health and Disease (9th ed., pp. 505–12). New York: Lippincott
Williams Wilkins.
Schoch, R.,Willoughby, D., & Greenwood, M. 2006. The regulation and expression of
the creatine transporter: A brief review of creatine supplementation in humans and
animals. Journal of the International Society of Sports Nutrition, 3 (1), 60–65.
Schroder, H., et al. 2002.The type, amount, frequency and timing of dietary supplement use
by elite players in the First Spanish Basketball League. Journal of Sports Science, 20 (4),353–58.
Shute, N. 2007. Over the limit? Americans young and old crave high-octane fuel, and
doctors are jittery. U.S. News & World Report (April 23), 60–68.
Spiering, B.A., et al. 2007.Responses of criterion variables to different supplemental doses
of l-carnitine l-tartrate. The Journal of Strength and Conditioning Research, 21 (1), 259–64.
Spriet, L.L. 1995. Caffeine and performance. International Journal of Sport Nutrition
(June, 5 Suppl.), S84–99.
Syrotuik, D.G., & Bell, G.J. 2004. Acute creatine monohydrate supplementation: A descriptive
physiological profile of responders vs. nonresponders. The Journal of Strength
and Conditioning Research, 18 (3), 610–17.
Wiles, J.D., et al. 2006.The effects of caffeine ingestion on performance time, speed and power
during a laboratory-based 1 km cycling time-trial. Journal of Sports Science, 24 (11), 1165–71.
Williams, M. 2005.Dietary supplements and sports performance: Amino acids. Journal
of the International Society of Sports Nutrition, 2 (2), 63–67.
