Heart Disease: Is There a Gender Divide?
Although many women worry about their risk of getting breast cancer, heart disease is actually the leading killer of females in America. Not only does heart disease kill more women than men each year (Thom et al. 2006), but females who survive a cardiac event fare much worse than their male counterparts (Blomkalns et al. 2005). Yet many women and their physicians fail to recognize the toll that cardiovascular disease (CVD) can take on the female body, and thus fail to do what is necessary to reduce the risk of getting this largely preventable disease (Mosca et al. 2005).
Now the latest research and recommendations are in: lifestyle modification is crucial (in fact, it trumps medical intervention) when it comes to preventing CVD in women. The American Heart Association’s (AHA) Evidence-Based Guidelines for Cardiovascular Disease Prevention in Women was updated and released this year (Mosca et al. 2007). These new guidelines present a major opportunity for fitness professionals to help women greatly reduce their risk of developing CVD.
This article provides a primer on how CVD develops in women; how the condition differs in women as opposed to men; how to recognize the risk factors and signs and symptoms in women; and how to understand and apply the latest recommendations and lifestyle modifications that will benefit your female clients. Further, it will provide practical tips and recommendations to empower fitness professionals to take action within their scope of practice.
What Is CVD?
The term cardiovascular disease refers to any disease of the heart and its blood vessels. Generally speaking, CVD is an umbrella term that encompasses all conditions affecting the heart muscle itself, the valves of the heart and/or the blood vessels that supply the heart (i.e., coronary arteries).
Vessel disease, or vascular disease, includes diseases such as hypertension (high blood pressure) and atherosclerosis (hardening of the arteries caused by the formation of plaque deposits within the arterial wall).
Heart disease is a complicated subject that exceeds the scope of this article; for a more thorough description of the different types of CVD, check out www.mayoclinic.com/health/cardio
vascular-disease/HB00032.
Atherosclerosis of the coronary arteries is the main culprit behind chest pain (angina) and heart attack (myocardial infarction). Although the condition is not usually dangerous until middle age and beyond, atherosclerosis typically begins to develop in childhood (Haust 1990; McMahan et al. 2006).
During the earliest stages of atherosclerosis, “fatty streaks” of oxidized cholesterol and lipid particles accumulate deep in the arterial wall. Due to the typical high-fat, low-fiber diet and sedentary lifestyle favored by the majority of Americans, the fatty streaks develop by the teenage years (McGill & McMahan 1998). Because these fatty streaks do not yet obstruct blood flow, there are no outward signs or symptoms of CVD.
Over time, however, a cholesterol plaque develops in the artery, which may become susceptible to rupture. This fibrous plaque tends to form in males by their 20s and in females by their 50s–60s. An advanced lesion, or complicated plaque, develops as the fibrous plaque continues to progress and becomes calcified. Males tend to develop lesions by age 30–40, whereas this occurs in females much later in life, usually by age 70. Often, the first sign of CVD in both men and women is a heart attack in which a lesion ruptures, forming a clot in the artery that completely obstructs blood flow (Fuster et al. 2005).
High blood cholesterol levels, particularly low-density lipoprotein (LDL) levels, coupled with oxidation of that cholesterol, are the main culprits in the development of atherosclerosis.
So why do women have a slower progression of artery-clogging plaques, but a higher total morbidity and mortality rate than men, even though a smaller percentage of women are affected by the disease (AHA 2007)? Women develop heart disease about 10–15 years later than men due to high levels of estrogen. Estrogen produced by the body is thought to help protect the heart because the hormone
- lowers dangerous LDL cholesterol levels;
- increases healthy high-density (HDL) cholesterol levels;
- reduces the progression of lesions; and
- dissolves clots (Klouche 2006).
After menopause, the levels of estrogen in a woman’s body drop, which increases the risk of CVD (Rosano et al. 2007). That’s partly why older age is considered a risk factor for heart disease in women after age 55, compared with age 45 for men. However, it is important to note that taking estrogen supplements does not protect the heart and might increase the risk of other serious conditions, such as breast cancer, stroke and blood clots (Manson et al. 2003; United States Preventive Services Task Force [USPSTF] 2005).
Even if women do get heart disease later in life than men, that doesn’t explain why they have worse outcomes and die more often from the disease than men do. While the reason for this disparity is still unknown, it may be partly because women tend to be older when they have a first heart attack and are thus more likely to die from it in the first few weeks following the event. But even this theory doesn’t account for all of the difference between outcomes and mortality rates. Some of the disparity may lie in how women are treated by the medical community.
Sad to say, but many physicians and women suffer from a lack of knowledge about the serious threat that CVD poses to females.
“Heart disease should top the list of women’s health concerns; unfortunately, it doesn’t even come close,” according to Sharonne Hayes, MD, director of the Mayo Clinic Women’s Heart Clinic at Mayo Clinic College of Medicine in Rochester, Minnesota. “Many women have a disproportionate fear of breast cancer and dutifully present for annual mammography while remaining oblivious to their risk of cardiovascular disease” (Hayes 2006).
This is borne out by the fact that only 57% of women in 2006 knew that CVD disease is the number-one killer for women, according to statistics provided by the National Heart, Lung, and Blood Institute (NHLBI 2007). Although that is an improvement from the 34% who were aware of this fact in 2000, it still isn’t nearly enough (NHLBI 2007).
When it comes to the medical community, many doctors themselves need some educating. Fewer than 1 in 5 physicians in 2004 knew that more women than men die of CVD each year (Mosca et al. 2005). Beyond a knowledge deficit, physicians also consistently perceive that there is a lower risk for CVD in women compared with men (Mosca et al. 2005).
Complicating this misunderstanding, many women and doctors also fail to recognize the early signs of an impending cardiovascular catastrophe. Unlike men, women often don’t experience the “typical” signs of heart disease, such as chest pain. When women patients do complain of chest discomfort, they often fail to describe it as pain in the chest, instead reporting an aching, tightness or pressure in the area. More often, women experience different symptoms than men—sometimes 4–6 months or more—before an actual heart attack or other cardiovascular event. These symptoms could include severe fatigue, sleep disturbances, shortness of breath, indigestion and anxiety (McSweeney et al. 2003). This disparity in signs and symptoms and terminology is important because physicians and emergency room personnel often assess primarily for chest pain when trying to rule out or rule in a heart attack.
Even when medical personnel do recognize that a woman might be experiencing CVD, their female patients often don’t get the treatment that they need. Women typically receive fewer cardiac procedures, such as catheterization and bypass surgery (Seils, Friedman & Schulman 2001); thrombolytic therapy to destroy blood clots (Grace et al. 2003); cardiac rehabilitation (Witt et al. 2004) or even prescriptions for drugs to treat CVD (Harrold et al. 2003).
Studies show that women also have worse in-hospital and long-term outcomes and increased hospital readmission following bypass surgery, unrelated to patient characteristics, such as presurgery health status or illness severity (Vaccarino et al. 2003). Many of these harmful outcomes can be improved or even prevented with increased research, awareness, advocacy and vigorous attempts at lifestyle change. Fitness professionals in particular are uniquely positioned to inspire such change in their female clients.
Educate Clients About Their Risk
As a fitness professional, you are committed to helping people to adopt healthier lifestyles. With your health and science knowledge, you also serve a critical role as a link between the lay consumer and the busy, time-constrained physician who often fails to provide crucial lifestyle recommendations (Mosca et al. 2005). Empower your female clients of all ages to minimize their CVD risk by educating them about the known risk factors and encouraging them to talk with their doctor about their own personal risk.
Some risk factors for CVD include
- elevated total and LDL cholesterol levels
- low HDL cholesterol levels
- obesity
- smoking
- hypertension
- sedentary lifestyle
- poor diet
- stress
- depression
- family history of premature CVD
- middle age
- diabetes (National Cholesterol Education Program Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults 2002; Mosca et al. 2007)
The more risk factors that are present, the higher the risk of atherosclerosis and subsequent heart attack or stroke. A simple preventive health check-up at the doctor’s office and a blood draw in the lab can arm a woman with the information needed to determine her specific risk. Give your clients a copy of “Questions to Ask Your Doctor,” below, to bring to their appointments.
Emphasize to clients the importance of closely monitoring the development of any of these risk factors. This is vital not only for older female clients who may have already developed one or more risk factors and now must vigorously work to reverse them or at least prevent their progression, but also to your younger clients who seem to be perfectly healthy.
“There appears to be a critical period in young adulthood to middle age, where if you avoid getting risk factors, you can almost abolish your risk of getting heart disease,” says Donald M. Lloyd-Jones, MD, associate professor of preventive medicine at Northwestern University’s Feinberg School of Medicine in Chicago, in an article that appeared in a recent issue of the Journal of the American Medical Association (Mitka 2007). “And while eliminating risk factors once they are present through lifestyle modification or medical therapy reduces your chances of getting heart disease, it doesn’t come anywhere close to the protection you have if you’ve never had the risk factors.”
Lloyd-Jones should know. He is the lead author of a study that found if you can make it to age 50 without experiencing these risk factors, your chance of developing heart disease is very low; only 8.2% of women with no risk factors developed CVD, compared to 50.2% of women who had 2 or more risk factors (Lloyd-Jones 2006). These results prove that it’s never too early to start your heart disease prevention lifestyle change.
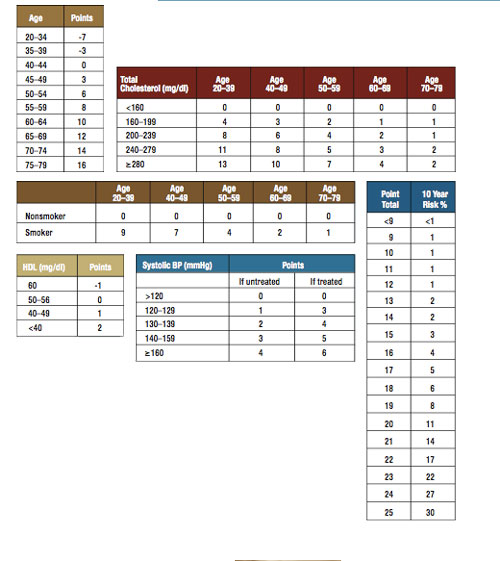
After your client visits her physician, ask if the doctor determined her risk stratification. The 2007 AHA guidelines encourage all women to be stratified as either “optimal risk,” “at risk” or “high risk” based on their risk factors (Mosca et al. 2007). This risk stratification helps determine the intensity of medication and lifestyle treatments necessary to lessen the odds of a future heart attack or cardiovascular-related death. See sidebar “How to Estimate Your Risk,” below, to view the tool physicians utilize to assess risk and determine CVD management.
If your client is determined to be at “high risk,” that means she has a greater than 20% chance of having a heart attack in the next 10 years (Mosca et al. 2007). People with pre-existing CVD and/or diabetes are automatically considered high risk. Clients who are at high risk are most in need of some serious and sweeping lifestyle modifications.
An “at risk” client has one or more risk factors for heart disease. While the chances are low that she will have a cardiovascular event in the next 10 years, her lifetime risk of heart disease is high, and she should initiate efforts to decrease the odds (Mosca et al. 2007).
“Optimal risk” means that a client has less than a 10% chance of experiencing a heart attack or coronary death in the next 10 years, based on the Framingham risk assessment tool (Mosca et al. 2007). While this sounds less dire than the other stratifications, it doesn’t mean she should pat herself on the back and treat the whole family to pepperoni pizza for dinner on a nightly basis. Rather, her goal should be to remain free of risk factors to age 50 and beyond so that she can drastically minimize her risk of ever developing CVD.
Regardless of risk stratification, all clients should be encouraged to follow these guidelines, with women at highest risk needing to make changes urgently:
Quit Smoking. Smoking is responsible for multiple serious diseases. A lean and physically fit, fruit- and vegetable-loving woman who smokes is not healthy and is not immune from CVD.
Aim for a Healthy Body Mass Index (BMI). A BMI of between 18.5 and 24.9 is considered optimal (check out www.nhlbisupport.com/bmi/ to determine your BMI). While this BMI range may be out of the question for many clients, even a 5%–10% weight loss reduces CVD disease risk (Tuomilehto et al. 2001).
Engage in Regular Exercise. Experts recommend getting at least 30 minutes of moderate-intensity physical activity daily. If your client needs to lose weight, up that time to 60–90 minutes daily. Help your clients plan ways to incorporate enjoyable and invigorating physical activities into their daily routine. Remind them that a simple brisk walk with their dog or with a friend after dinner counts.
Participate in a Cardiac Rehabilitation Program. This program can be in-hospital or a physician-guided home- or community-based exercise training program. Clients who have had a recent acute coronary syndrome or coronary intervention, new-onset or chronic chest pain, recent stroke, peripheral vascular disease or symptoms of heart failure need cardiac rehab to prevent a future event.
Eat a Healthy Diet. Aim for a regular diet rich in fruits and vegetables, whole grains and high-fiber foods. Consume fish (in particular oily fish like salmon, trout and tuna) at least twice per week; limit saturated fat, cholesterol, alcohol and sodium intake. Avoid any foods that contain trans fats. Advise clients to check out the MyPyramid website (www.mypyramid.gov), which offers many resources to help people get started. If more help is needed, refer your clients to a registered dietitian.
Seek Help for Depression. Depression wreaks havoc on the heart and arteries. If your client has depression that doesn’t improve with a regular exercise program, strongly encourage her to seek professional help not only for her mental health, but also to protect her heart.
While all of these strategies may sound fairly straightforward, keep in mind that only 3% of Americans eat healthfully, engage in regular physical activity, maintain a healthy weight and don’t smoke (Sandmaier 2007). That leaves a lot of room for fitness professionals to make a difference. For more tips, see “10 Ways to Educate Female Clients About CVD” below.
Heart disease robs women of their quality of life and can be deadly. The clock is ticking for all women—regardless of age, risk factor status, race or socioeconomic status—to take action. As a fitness professional, you can inspire women around the world to embrace fitness, wholesome nutrition and a healthy heart.
Encourage your clients to take this list to their physician’s office; the answers to these questions will provide vital information needed to optimize heart health.
- What is my risk for heart disease?
- What is my blood pressure reading? What does this reading mean for me, and what do I need to do about it?
- What are my cholesterol numbers? These should include total cholesterol, LDL (or “bad”) cholesterol, HDL (or “good”) cholesterol and triglycerides. What do these numbers mean for me, and what do I need to do about them?
- What is my body mass index (BMI) and my waist circumference measurement? Do these numbers indicate that I need to lose weight?
- What is my blood sugar level? Does it mean that I’m at risk for diabetes?
- What other screening tests for heart disease do I need? How often should I return for checkups for my heart health?
- What tools can I employ to quit smoking?
- How much physical activity do I need to help protect my heart?
- What is a heart healthy eating plan for me? Should I see a registered dietitian to learn more about healthy eating?
- How can I tell if I’m having a heart attack? What are the typical signs in a woman compared with a man?
Source: “Heart Healthy Handbook for Women” by the National Heart, Lung, and Blood Institute; National Institutes of Health; United States Department of Health and Human Services (www.hearttruth.gov). Available at www.nhlbi.nih.gov/health/hearttruth/material/NHLBI_3942_HHH_041707.pdf.

Share these strategies with your female clients to help increase awareness of their risk of developing cardiovascular disease:
- Get the Word Out to Clients. Go to the Heart Truth website (www.hearttruth.gov) and order your red dress pin, which is used to educate the public about the toll that heart disease takes on women. Then wear your pin to work, and tell everyone who asks (and even some who don’t) what it signifies. This can lead to a discussion of other ways to reduce the risk of CVD.
- Provide Clients With Pamphlets on Heart Health. Order several copies of the “Healthy Heart Handbook for Women” from the hearttruth.gov website, and display them prominently in your facility. You might put a few copies in the magazine rack by your cardio machines, in the locker room or at the front desk near the fitness class schedule.
- Offer Free Risk Factor Screening at Your Facility. Measure fasting lipoprotein profile, blood pressure, fasting blood glucose, waist circumference and BMI. Make sure you tell participants what these numbers mean and how they can take action to decrease their risk.
- Encourage Clients to See Their Doctor for a Risk Factor Assessment. Ask them to bring you their results so you can help them stick to a plan. You can also use the results to modify their exercise program to further help reduce their risk. When speaking to their physician, remind clients to speak up and ask questions about their risk of developing heart disease and ways to reduce that risk.
- Offer an Educational Seminar on Women and Heart Disease. The website hearttruth.gov offers a speaker’s kit that provides all the materials and information you will need.
- Communicate With Your Clients’ Other Healthcare Providers. With your client’s permission, ask her doctor for a risk factor assessment and recommendations and contraindications for an exercise program. On a quarterly basis, fax the physician quarterly progress reports that show the client’s progress and fitness level. This communication will prompt the doctor to ask the client about improvements in physical activity and weight loss and will also make it more likely that the physician will closely monitor the woman’s CVD risk factor status.
- Wear Red to Show Your Support. National Wear Red Day is February 1, 2008. You can make this event a day of recognition and education at your club. The American Heart Association campaign called National Go Red for Women has developed a list of materials that you will need; access this list at www.goredforwomen.org.
- Become a Volunteer Advocate for Heart Health. Offer your services and expertise pro bono to women in your community who may be at risk for heart disease but cannot afford to join a health club.
- Walk the Walk. Be a good role model and learn about your own personal risk of heart disease. Educate your own mom, wife, sister, daughters, neighbors, coworkers and all female clients about heart health, and work vigorously to change modifiable risk factors.
- Continue Doing What You Do Best. Your efforts to help your clients develop a safe, enjoyable and effective exercise program is critically important to help them reduce their risk of CVD. Know that your work is incredibly important, and continue your tireless efforts to help women adopt an active and healthier lifestyle.
- The National Heart, Lung, and Blood Institute’s (NHLBI) The Heart Truth (www.hearttruth.gov). This national awareness campaign informs women about the risk of heart disease. The website includes a link to the “Healthy Heart Handbook for Women” for download or purchase ($4). The handbook provides a comprehensive update of the latest knowledge of women and heart disease as well as practical tips to reduce risk.
- The NHLBI “Your Guide to Better Health” (http://hp2010.nhlbihin
- .net/yourguide). This series includes a guide on living with heart disease, lowering blood pressure through diet; lowering cholesterol levels; and increasing physical activity.
- American Heart Association (www.americanheart.org). The AHA is the leading organization devoted to the prevention and treatment of heart disease; this website provides myriad resources and opportunities to improve heart health.
- Society for Women’s Health Research (www.womenshealth research.org). Check out the comprehensive statistics on gender differences in cardiovascular disease.
- WomenHeart. The National Coalition for Women with Heart Disease (www.womenheart.org) is a patient advocacy organization devoted to providing resources and support to women with heart disease.
- Heart Healthy Women (www.hearthealthywomen.org). This highly reputable online source provides educational resource for patients and healthcare providers.
- Sister to Sister Foundation (www.sistertosister.org). This nonprofit organization is dedicated to prevent heart disease in women; the organization provides free cardiovascular screening and education.
Natalie Digate Muth, MPH, RD, CSCS, is a registered dietitian and medical student at the University of North Carolina, Chapel Hill. As part of her training, she is currently conducting research on cholesterol and CVD risk at the University of California, San Diego. She is also a master trainer for the American Council on Exercise.
References
Blomkalns, A.L. et al. 2005. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: Large-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. Journal of the American College of Cardiology, 45, 832–37.
Fuster, V. et al. 2005. Atherothrombosis and high-risk plaque.Journal of the American College of Cardiology, 46, 937–54.
Grace, S.L. et al. 2003. Presentation, delay and contraindication to thrombolytic treatment in females and males with myocardial infarction. Women's Health Issues, 13 (6), 214–21.
Harrold, L.R. et al. 2003. Age and sex differences in the treatment of patients with initial acute myocardial infarction: A community-wide perspective. Cardiology, 99 (1), 39–46.
Haust, M.D. 1990. The genesis of atherosclerosis in pediatric age-group. Pediatric Pathology, 10 (1–2), 253–71.
Hayes, S.N. 2006. Identification of women with heart disease: A missed opportunity. Nature Clinical Practice, 3 (10), 522–23.
Klouche, M. 2006. Estrogens in human vascular diseases. Annals of the New York Academy of Science, 1089, 431–43.
Lloyd-Jones, D.M. et al. 2006. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation, 113, 791–98.
Manson, J.E. et al. 2003. Estrogen plus progestin and the risk of coronary heart disease. The New England Journal of Medicine, 349 (6), 523–34.
McGill, H.C. & McMahan, C.A. 1998. Determinants of atherosclerosis in the young. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. American Journal of Cardiology, 82 (10B), 30T–36T.
McMahan, C.A. et al. 2006. Pathological determinants of atherosclerosis in youth risk scores are associated with early and advanced atherosclerosis. Pediatrics, 118 (4), 1447–55.
McSweeney, J.C. et al. 2003. Women’s early warning symptoms of acute myocardial infarction. Circulation, 108 (21), 2619–23.
Mitka, M. 2007. A change of heart guidelines for women. Journal of the American Medical Association, 297 (13), 1421–22.
Mosca, L. et al. 2005. National study of physician awareness and adherence to cardiovascular disease prevention guidelines. Circulation,111, 499–510.
Mosca, L. et al. 2007. Evidence-based guidelines for cardiovascular disease prevention in women: 2007 update. Circulation, 115, 1481–1501.
National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). 2002. Bethesda, MD: U.S. Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Institute.
National Heart, Lung, and Blood Institute (NHLBI). 2007. What Is the Heart Truth?; retrieved from www.nhlbi.nih.gov/health/hearttruth. on July 18, 2007.
Rosano, G.M. et al. 2007. Menopause and cardiovascular disease: The evidence. Climacteric, 10 (Suppl 1), 19–24.
Sandmaier, M. 2007. The Healthy Heart Handbook for Women. Bethesda, MD: U.S. Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Insitute; retrieved from www.nhlbi.nih.gov/health/ public/heart/other/hhw/hdbk_wmn.pdf. on July 18, 2007.
Seils, D.M., Friedman, J.Y., & Schulman, K.A. 2001. Sex differences in the referral process for invasive cardiac procedures. Journal of the American Medical Women's Association, 56 (4), 151–54.
Thom, T. et al. 2006. Heart disease and stroke statistics—2006 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation, 113 (6), e85–e151.
Tuomilehto, J. et al. 2001. Prevention of Type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. New England Journal of Medicine, 344, 1343–50.
United States Preventive Services Task Force (USPSTF). 2005. Hormone therapy for the prevention of chronic conditions in postmenopausal women: Recommendations from the United States Preventive Services Task Force. Annals of Internal Medicine, 142, 855–60.
Vaccarino, V. et al. 2003. Gender differences in recovery after coronary artery bypass surgery. Journal of the American College of Cardiology, 41(2), 307–314.
Witt, B.J. et al. 2004. Cardiac rehabilitation after myocardial infarction in the community. Journal of the American College of Cardiology, 44 (5), 988–96.
