
Heart Rate Variability & Overtraining
Can New Research Prevent an Age-Old Paradigm?
Heart rate variability (HRV) is a reliable marker of physiological factors that directly affect the rhythms of the heart (Acharya et al. 2006). Acharya and colleagues explain that HRV reflflects the heart’s ability to adapt to changing circumstances—stress, exercise and disease—by balancing the regulation of the autonomic nervous system, which controls bodily functions such as breathing, heart-beat and digestion.
Exercise training status, including overtraining, can play a key role in HRV (Achten & Jeukendrup 2003). Chronic overtraining often leads to physiological and psychological symptoms that impair performance and can delay full recovery for weeks or more (Meeusen et al. 2013). For personal trainers, an understanding of the relationship between HRV and overtraining, including a deeper grasp of the potential mechanisms and prevention strategies of over-training, is paramount for helping clients achieve optimal gains in cardiorespiratory effifficiency.
What is HRV, and What Does It Tell Us?
HRV describes fluctuations in consecutive heartbeat intervals above and below an average heart rate over a period of time; in clinical settings, the measurement time might range from 5 minutes to 24 hours (Acharya et al. 2006). HRV is particularly influenced by the autonomic nervous system (Acharya et al. 2006), which comprises the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS).
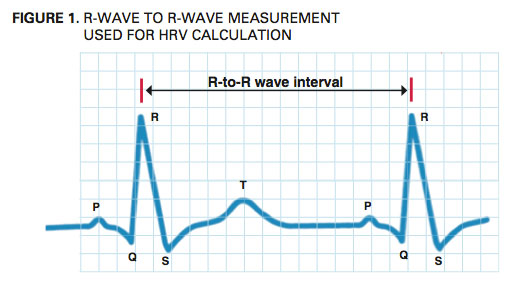
The SNS mobilizes the body’s hormones and nerves to respond speedily to exercise, stress and fight- or-flight situations—enabling a person to run across the street quickly to avoid an oncoming car, for example, or to respond swiftly to the onset of a thunderstorm. Conversely, the PNS has a slowing effect on heart rate, which helps the body to conserve energy; this system plays a strong role in bodily function homeostasis, including digestion and gland activity. The unique and different contributions of the SNS and PNS mildly modify the intervals between heartbeats, or HRV (see Figure 1).
For scientists, coaches and personal trainers, HRV measurements—called R-to-R wave intervals—are useful markers for understanding the status of the autonomic nervous system and can be used to clinically detect cardiac health and client readiness for intensity and volume progressions in exercise training.
Clinical Applications of HRV Analysis
Acharya et al. (2006) say HRV measurements are noninvasive and most reliable when performed under standardized conditions. Research suggests that low HRV is a negative outcome of cardiovascular diseases, diabetic neuropathy, elevated blood pressure and heart attack (Stauss 2003). HRV is also useful in observing people with diabetes, which can cause severe dysfunction of the autonomic nervous system (Acharya et al. 2006). Low HRV may point to the onset of diabetic neuropathy, a complication of diabetes mellitus characterized by widespread breakdown of small nerves in the sympathetic and parasympathetic nerve tracts (Malik et al. 1996).
Smoking and alcohol consumption also affect HRV. Acharya and colleagues (2006) conclude that smokers have a depressed HRV, possibly a direct effect of how smoking impairs cardiovascular function, which the autonomic nervous system regulates (Archarya et al. 2006). Malpas, Whiteside & Maling (1991) studied HRV in 23 alcohol-dependent men and found it was significantly lower than in the non-alcoholic (healthy) control group.
HRV and Exercise: New Technologies
Some new technologies such as www.omegawave.com and www .bioforcehrv.com are using HRV to evaluate athletes’ readiness for exercise performance. Smartphone apps with heart rate monitors can measure HRV readily and conveniently, which means coaches, personal trainers and clients can easily monitor the cardiac, metabolic and central nervous systems to more accurately determine the best times to overload with intensity and/or workload volume and the best times to focus on recovery.
This allows personal trainers and coaches to better balance training progressions and recovery to avoid overtraining and declining performance. While HRV technologies were developed to identify risk levels for cardiac death and diabetic neuropathy, today they are gaining great interest and use in sports physiology and exercise. The main goal of the latest HRV technology is to promote positive overload and adequate recovery, preventing the deleterious effects of overtraining (Pichot et al. 2002). A deeper understanding of overtraining prevention is evolving, which may in turn lead to higher levels of successful training.
Overtraining in Exercise
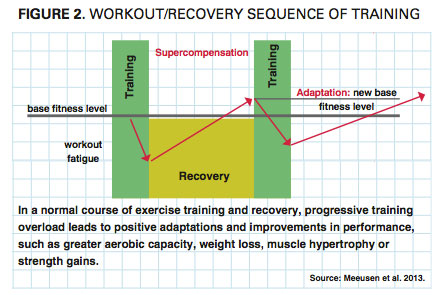
Personal trainers regularly monitor clients’ physiological and psychological responses to progressive overloads during a training program. After sufficient recovery from training fatigue, the body compensates by building strength and improving performance (see Figure 2).
Overtraining can be an unfortunate consequence of uncontrolled progressive overload. Some people believe overtraining is unique to trained, elite athletes, but trainers need to set clients straight: Successful training includes overload, but not in excess, and it requires adequate recovery, which many clients sacrifice in their quest for immediate results.
How to Define Overtraining
The phenomenon of overtrain- ing syndrome, often called “burn- out” or “staleness,” has motivated many researchers to investigate its causes and consequences. First, the researchers had to decide on a common title—in the past, OTS was called underperformance syndrome and sports fatigue syndrome (Armstrong & VanHeest 2002). To provide researchers and practitioners with standard language, Meeusen et al. (2013) recently proposed the following terminologies and definitions (see Figure 3).

- Overtraining is a process of intensified training leading to possible short-term outcomes of overreaching (called functional overreaching), extreme overreaching (called nonfunctional overreaching) or overtraining syndrome.
- Functional overreaching is a short period of increased training leading to a temporary performance decline. With satisfactory recovery, overreaching can lead to what Meeusen et al. (2013) call a “supercompensation” effect of enhanced performance.
- Nonfunctional overreaching is a longer process of intense training leading to stagnation and sustained performance decline that can last weeks or months (Meeusen et al. 2013). However, full recovery happens after satisfactory rest.
- Overtraining syndrome is a “prolonged maladaptation” that disrupts hormonal, biological and neurological regulatory mechanisms; these physiological consequences are accompanied by mood disturbances (Meeusen et al. 2013). Uniquely, Armstrong and VanHeest (2002) observe that OTS and clinical depression involve remarkably similar signs and symptoms, brain structures, neurotransmitters, endocrine pathways and immune responses.
What Overtraining Looks Like
A plethora of research has focused on identifying and assessing the physiological and psychological changes associated with overtraining, but not all studies measure the same variables, and those that do don’t always find the same results.
It is therefore important to note that no single overtraining marker or group of overtraining markers has been identified for a positive diagnosis of overtraining (Meeusen et al. 2013). Initially, there is some decline in performance. As presented in Figure 4, several common signs and symptoms
are associated with overtraining.
Armstrong & VanHeest (2002) say that with endurance sports, OTS is characterized by persistent fatigue and apathy. The authors also note that fatigue is associated with illnesses such as anemia, Lyme disease, mononucleosis, hypoglycemia, hypothyroidism
and chronic fatigue syndrome.
Several changes in the blood are observed with OTS, including decreases in hematocrit (the ratio of the volume of red blood cells to the total volume of blood), hemoglobin, iron and ferritin (Armstrong & VanHeest 2002). Ferritin is a protein that stores iron. Its levels can be used to measure the body’s iron levels indirectly. Low levels of ferritin are seen when iron is deficient. With insufficient iron, the body cannot produce enough hemoglobin, the component of red blood cells that carries oxygen. Iron deficiency anemia may result, raising the likelihood of fatigue, dizziness and elevated resting heart rate from overtraining
(Wyatt, Donaldson & Brown 2013).
Wyatt, Donaldson and Brown (2013) say testosterone levels decline with OTS. Testosterone serves a vital role in the body as an anabolic agent that boosts growth in tissues. Testosterone also promotes many metabolic activities, including the
stimulation of protein synthesis and red cell production. The authors say that lower testosterone levels lead to less protein synthesis and decreased production of red blood cells, thus delaying recovery from exercise. OTS also changes the concentration of other hormones, such as norepinephrine, epinephrine, hemoglobin, cortisol and leptin (Wyatt, Donaldson & Brown 2013).
With immune function, one area of interest with OTS is glutamine, the most abundant free amino acid in the body. Glutamine is produced in the muscles and is used extensively by the cells of the immune system to support production of lymphocytes, white blood cells that defend the body against cancerous cells, pathogens and foreign matter. Wyatt, Donaldson & Brown (2013) say that the lower glutamine levels observed with OTS weaken immune function by altering the function of lymphocytes.
Note: Signs and symptoms of overtraining are highly individualized and subjective, so they cannot be universally applied.
How to Prevent Overtraining Syndrome

Exercise professionals must remember that the underlying causes of overtraining are not fully understood. Clients who are struggling with anemia often present similar symptoms to those who are overtraining. The OTS Indicator Checklist (see sidebar) has been adapted from the OTS consensus statement article by Meeusen et al. (2013). Personal trainers can use this checklist to help identify or prevent OTS in clients. It is commonly accepted that the presence of one or more symptoms is sufficient to alert a personal trainer that a client may be overtraining (Wyatt, Donaldson & Brown 2013).
Meeusen and colleagues (2013) suggest that personal trainers and coaches must try to exclude organic disease as the cause of declining performance. Possibilities include
allergies, anemia, infectious diseases, eating disorders, adult-onset asthma, cardiovascular system conditions, diabetes, thyroid problems, adrenal gland problems and any biological abnormalities. Exercise professionals may need to encourage clients to see a doctor to rule out any of these illnesses. Also, Meeusen et al. (2013) emphasize that athletes require adequate rest and sufficient sleep. The absence of one full passive recovery day each week (during intensified training) is closely related to the signs of overtraining, according to these authors.
Final Thoughts on HRV and Overtraining
With advances in HRV, personal trainers can now non-invasively monitor the cardiac, metabolic and central nervous systems to better determine when it is appropriate to overload with intensity and/or workload (or both), and when it is best to train more lightly and focus on recovery.
Clients with overtraining syndrome will likely display one or more of the following: disrupted heart rate variability, performance declines, persistent fatigue, hematologic changes, hormone concentration changes, impaired immune function, persistent muscle soreness, loss of body mass, apathy, lack of motivation, loss of appetite, sleep disturbances (restless sleep), high stress levels, irritability, depression, attitude changes and a tendency to become easily distracted. Relieving overtraining may be aided by reducing daily training volume or intensity, resolving conflicts that may be adding stress, improving diet and/or taking a recovery break from training if conditions are problematic.
